A Practice-Based Observational Report, 2018 to January 2026
By Tony Jacobsen
Published July 2026
Version 1.0
Abstract
Adults with Osteogenesis Imperfecta, also known as O.I. or brittle bone disease, have limited access to exercise guidance that addresses progression, adaptation, confidence, and long-term participation. Much of the available information focuses on fracture prevention, physical limitations, pediatric care, or general recommendations to remain active.
This practice-based observational report summarizes community exercise coaching delivered between 2018 and January 2026. Approximately 50 adults with O.I. participated in one-on-one coaching during this period, with additional participation in group-based programming. Formal weekly self-reported data collection began within the Stronger Bones Coaching Group in November 2024.
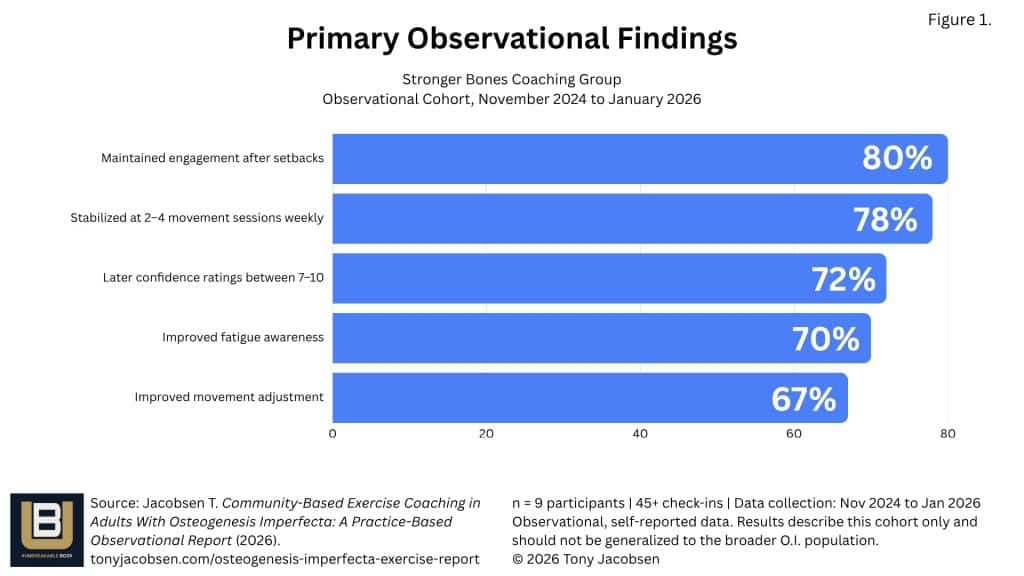
Between November 2024 and January 2026, nine participants submitted more than 45 structured check-ins. Observed trends included greater movement consistency, increased confidence, improved awareness of fatigue and body signals, and continued engagement through injuries, illness, stress, and other disruptions. No fractures occurred during supervised live exercise sessions between 2018 and January 2026.
These findings are observational and self-reported. There was no control group, no standardized clinical assessment, and no collection of medical endpoints such as bone mineral density. The findings do, however, offer a community-based perspective on the feasibility and sustainability of structured, adaptive exercise for adults with O.I.
Practice Note
This report describes observations from community-based coaching rather than outcomes from a controlled research study. It is intended to contribute to discussion and generate opportunities for future research, not to establish clinical recommendations.
Why This Report Was Created
Exercise guidance for people with Osteogenesis Imperfecta has historically emphasized precaution.
That caution is understandable. O.I. is a connective tissue disorder most commonly associated with fragile bones and increased fracture risk. Depending on the individual, it may also affect muscle strength, joint stability, fatigue, balance, pain, mobility, hearing, breathing, and other aspects of daily life.
However, caution without a clear pathway forward can leave adults with O.I. knowing what they have been advised not to do, but unsure how to safely begin, adapt, or progress.
There remains limited adult-focused information about how people with O.I. engage with structured exercise in everyday settings. There is even less community-based data examining movement consistency, confidence, self-regulation, functional change, and sustained participation over time.
This report was created to document what has been observed through real-world coaching and to identify questions that deserve more formal scientific investigation.
It is not a clinical trial. It is a practice-based observational summary developed from coaching experience, participant feedback, testimonials, and structured weekly self-reported check-ins.
Coaching Background, 2018 to October 2024
Beginning in 2018, approximately 50 adults with Osteogenesis Imperfecta participated in individualized online coaching.
The typical coaching relationship during this period lasted approximately four months. Coaching was usually delivered through two to three 45-minute sessions per week, depending on the participant’s goals, availability, health, and current capacity.
Participants ranged in age from their mid-20s through their 70s. The most represented age group was approximately 45 to 70. Most participants identified as having Type 1 O.I., although Types 2, 3, and 4 were also reported. Some participants did not identify their specific O.I. type.
Because the coaching was conducted online, participation extended across more than half of the United States and included international participants from Europe, Australia, India, and other parts of Asia.
During this early period, data collection was not standardized. Outcomes were documented primarily through participant feedback, direct communication, testimonials, and observations made during coaching sessions.
These qualitative reports included improvements in movement confidence, daily function, mobility, pain management, consistency, nutrition habits, mood, and independence. Because these outcomes were not collected through a consistent research protocol, they should be viewed as testimonials and practice observations rather than formal comparative data.
The Stronger Bones Coaching Group
The Stronger Bones Coaching Group began in fall 2024, with formal weekly self-reported data collection starting in November 2024.
This introduced a more consistent structure for tracking how participants were moving, how confident they felt, how they responded to fatigue and discomfort, and how they adjusted their activity during changing health or life circumstances.
The group included a weekly 30-minute live exercise session and a monthly one-hour coaching call. Participants could also ask questions and receive direct support between scheduled sessions.
From November 2024 through January 2026, nine unique participants submitted more than 45 structured weekly check-ins.
The check-ins tracked:
- Intentional movement sessions completed each week
- Self-reported confidence in movement
- Awareness of pain, fatigue, and other body signals
- Ability to adjust or modify movement when needed
- Qualitative observations about function, habits, setbacks, and progress
The full check-in format, internal coaching processes, programming decisions, and raw participant-level data are not included in this public report. Additional de-identified information may be considered as part of an appropriate academic, clinical, or organizational collaboration.
Exercise Intervention Overview
The coaching model was not limited to resistance training.
Programming used an adaptive, multi-component approach that incorporated strength, cardiovascular conditioning, mobility, flexibility, and movement awareness. Sessions were designed to support seated or standing participation, depending on the individual.
Equipment could include body weight, a chair, resistance bands, or dumbbells. Participants were encouraged to work within their current abilities and adjust according to how their bodies were responding.
Exercises were demonstrated in adaptable formats during live online sessions. The coaching environment emphasized awareness, participation, sustainability, and individual choice rather than comparison or pressure.
The purpose was not to push every participant toward the same physical standard. It was to help each person develop a more consistent and informed relationship with movement.
Safety considerations included controlled movement, individualized adaptation, reduced repetition when appropriate, and avoidance of ballistic exercise. These are broad principles rather than a complete description of the programming or coaching methodology.
Across approximately eight years of supervised live coaching, no fractures were reported or observed during scheduled exercise sessions.
This observation should not be interpreted as proof that the program eliminates fracture risk. It indicates that no fractures were reported or observed during the live supervised sessions included in this period.
Observational Findings
Movement Consistency
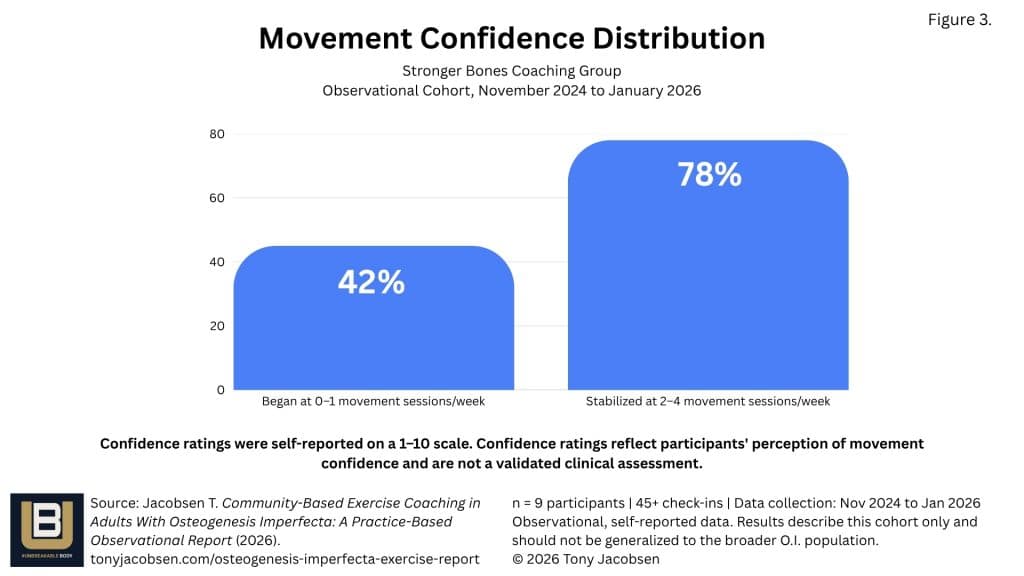
At the beginning of the structured observation period, approximately 45% of participants reported completing zero or one intentional movement session per week.
Over time, approximately 78% stabilized at two to four movement sessions per week. The group-wide average was 2.7 sessions per week.
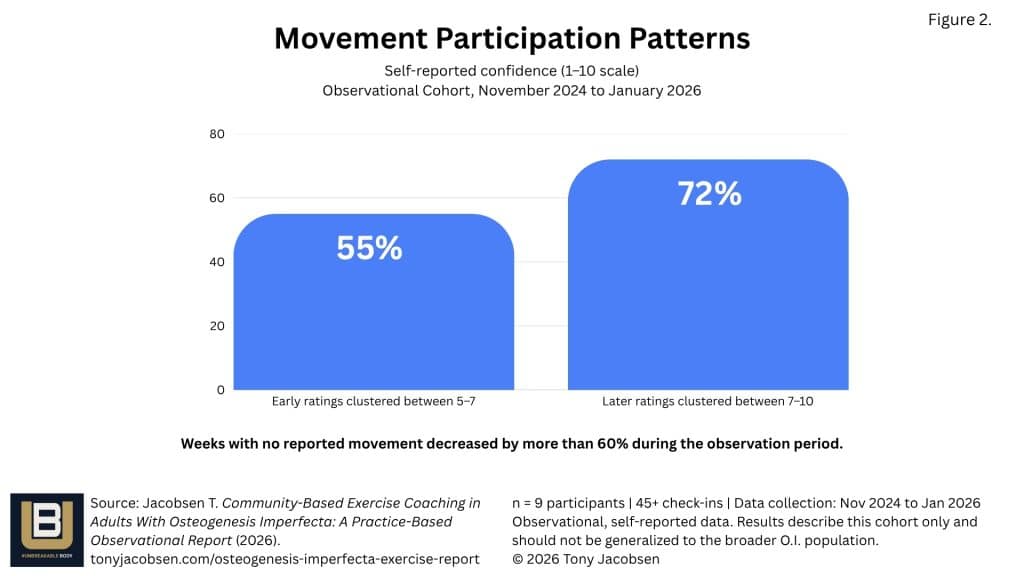
Weeks in which participants reported no intentional movement decreased by more than 60% over the observation period.
This suggests that many participants moved from inconsistent or reactive activity patterns toward more repeatable weekly engagement.
The importance of this shift is not simply the number of sessions completed. Consistency creates more opportunities to build awareness, confidence, skill, and familiarity with movement.
Confidence in Movement
Participants rated movement confidence on a scale from 1 to 10.
Early confidence responses most commonly fell between 5 and 7. Later in the observation period, approximately 72% of confidence ratings fell between 7 and 10.
Participants also appeared to regain confidence more quickly after interruptions caused by injury, illness, stress, or other setbacks.
This may indicate increasing self-trust and a greater understanding of how to return to movement without expecting an immediate return to previous capacity.
Ability to Adjust Movement
Across the structured check-ins, approximately 67% of responses indicated that participants noticed positive changes in their ability to adjust movement when needed.
Later check-ins included more descriptions of proactive modifications, such as changing intensity, reducing range of motion, selecting a different exercise, or responding earlier to discomfort and fatigue.
This is an important observation because long-term participation may depend not only on the ability to complete an exercise, but also on the ability to recognize when and how it should be changed.
Fatigue Awareness and Self-Regulation
Fatigue remained present throughout the observation period, as would be expected within a population living with a chronic condition.
However, approximately 70% of participants reported becoming more aware of body signals before fatigue or discomfort escalated.
Earlier check-ins were more likely to describe fatigue as disruptive or as a reason to stop participating. Later responses more often described fatigue as something that could be recognized, managed, and accommodated.
The goal was not to remove fatigue. It was to help participants respond to it with greater awareness and flexibility.
Participation Through Setbacks
During the observation period, participants experienced fractures, surgeries, illness, seasonal depression, travel, personal stress, and other disruptions.
Despite these challenges, approximately 80% continued submitting check-ins after an injury or setback. Many maintained at least two movement sessions per week during periods of recovery, using appropriate adjustments based on their circumstances.
This does not mean every participant remained equally active at all times. It suggests that participation became less dependent on ideal conditions.
Rather than treating a setback as the end of the process, participants increasingly found ways to remain connected to movement in a form that made sense for that period.
Functional and Quality-of-Life Observations
Participants described changes that extended beyond structured exercise sessions.
Reported functional improvements included greater confidence with daily activities, improved balance, increased strength for household tasks, more independent mobility, and a reduced fear of movement.
One participant reported being able to walk without crutches or a walker for more than three-quarters of the day. The same participant described improved strength during ordinary activities, including lifting several plates from the dishwasher at one time.
Another participant described discovering that exercise was possible even on mornings when pain was present.
Others reported rebuilding an exercise habit, feeling more connected to the O.I. community, becoming more aware of nutrition, and feeling more capable in their bodies.
One former coaching client described remaining healthier and more mobile three years after beginning the individualized plan developed during coaching. Another reported losing 12 kilograms after applying recommendations related to movement and nutrition.
These accounts should not be treated as evidence that the same outcomes will occur for every participant. They illustrate the types of changes individuals considered meaningful in their own lives.
Social and Emotional Observations
Participants also reported emotional and social changes alongside their movement progress.
Common themes included improved mood, reduced anxiety, increased motivation, stronger community connection, and a greater sense of independence.
Words and phrases such as “motivated,” “energized,” “stronger,” “more connected,” and “more confident” appeared regularly in participant responses.
For people who have spent years being told to be careful, movement can carry emotional weight. Fear of pain, fear of fracture, previous medical experiences, and uncertainty about what is safe may all affect participation.
A community-based model may help reduce isolation by allowing participants to see other people with O.I. moving, adjusting, resting, returning, and progressing in different ways.
Enjoyment may also matter. Although this report did not formally measure enjoyment as an outcome, sessions were intentionally designed to be engaging, supportive, and approachable. Future research could examine whether enjoyment and community connection contribute to adherence among adults with O.I.
Interpretation
These observations suggest that structured, adaptive, multi-component exercise is feasible for adults with Osteogenesis Imperfecta.
The Stronger Bones Coaching Group data also suggest that this type of support may be sustainable. Participants increased or maintained movement frequency, reported greater confidence, developed stronger self-regulation skills, and remained engaged through significant disruptions.
The results do not establish that coaching caused each reported improvement. They also do not establish that the program changes bone density, prevents fractures, or produces a specific medical outcome.
They do support a broader conclusion: adults with O.I. may benefit from access to exercise support that goes beyond general advice to “stay active” or “be careful.”
A structured pathway that includes options, progression, supervision, community, and participant choice may represent an important and currently underserved component of adult O.I. support.
For adults living with O.I., consistency may be as meaningful as intensity. A movement practice that people are willing and able to sustain over time may offer greater long-term value than programs that cannot be maintained.
For this population, sustainable movement may contribute to function, confidence, independence, social connection, and overall quality of life.
That possibility deserves closer study.
Limitations
This report has several important limitations.
The Stronger Bones Coaching Group cohort was small, with nine unique participants included in the structured analysis. Data were self-reported and collected as part of a coaching program rather than a controlled research study.
There was no control group, randomization, blinded assessment, or standardized clinical testing. The program did not track bone mineral density, fracture incidence outside supervised sessions, medical biomarkers, or validated quality-of-life measures.
The percentages presented in this report describe patterns within the available check-in data. They should not be generalized to the entire O.I. population.
Data collected before November 2024 were primarily qualitative and included testimonials, participant feedback, and coaching observations. They were not gathered using the same weekly tracking process introduced through the Stronger Bones Coaching Group.
Participation duration, O.I. type, mobility level, health history, access to medical care, and individual goals varied among participants.
These limitations prevent causal conclusions. They do not erase the value of the observations, but they define how those observations should be interpreted.
Opportunities for Clinical and Research Collaboration
This observational report highlights several areas where collaboration between community practitioners, clinicians, and researchers could meaningfully expand the evidence base for adults living with Osteogenesis Imperfecta.
1. Biological Outcomes
Potential collaborations examining:
- Bone mineral density
- Muscle strength
- Balance
- Functional performance
2. Behavioral Outcomes
Potential collaborations examining:
- Exercise adherence
- Movement confidence
- Self-efficacy
- Fear of movement
- Recovery following fracture
3. Quality of Life
Potential collaborations examining:
- Independence
- Social connection
- Mental health
- Community participation
- Long-term sustainability
Through #UNBREAKABLE BODY, an established community of adults with Osteogenesis Imperfecta is already engaged in structured movement programming and ongoing participant communication. This creates opportunities for future collaborative studies that combine community implementation with academic research methodology.
Invitation for Collaboration
This report is intended to begin a conversation between the O.I. community, exercise professionals, researchers, clinicians, and organizations interested in adult health and quality of life.
Potential areas of collaboration include program evaluation, study design, participant-reported outcome measurement, adult O.I. exercise guidance, professional education, and research examining the physical and psychosocial effects of structured movement.
De-identified participant information may be considered for appropriate collaborations with clear expectations regarding data use, participant privacy, attribution, intellectual property, publication, and the role of the coaching program.
The deeper coaching framework, progression process, curriculum, session design, and internal program systems remain proprietary to #UNBREAKABLE BODY.
Researchers, clinicians, universities, medical organizations, and rare disease organizations interested in discussing this work are invited to connect.
Contact:
Tony Jacobsen
www.tonyjacobsen.com
Conclusion
Adults with Osteogenesis Imperfecta are often given clear information about risk, but far less information about how to build a sustainable movement practice.
This practice-based observational report suggests that adults with O.I. can participate in structured, adaptive, multi-component exercise over time. It also suggests that the value of exercise may extend beyond physical performance.
Participants reported greater consistency, confidence, body awareness, functional strength, social connection, and engagement through setbacks. No fractures occurred during supervised live sessions between 2018 and January 2026.
These findings do not prove clinical effectiveness or establish safety for every person with O.I. They do demonstrate that carefully supported exercise is possible, that continued participation can be sustainable, and that adults with O.I. need clearer pathways for movement that support function and quality of life.
The next step is collaboration.
Community experience can identify the questions. Scientific research can help answer them.
About the Author
Tony Jacobsen is an Adaptive Fitness Specialist, NASM Certified Personal Trainer, author, and board member of the Osteogenesis Imperfecta Foundation. Living with O.I. himself, he has spent more than eight years coaching adults with Osteogenesis Imperfecta through structured, adaptive movement and exercise. He is the founder of #UNBREAKABLE BODY, an online movement community designed to help people with disabilities, limited mobility, and fragile bones build greater confidence, strength, and independence through sustainable movement.
About This Report
This report represents a practice-based observational summary of community exercise coaching delivered between 2018 and January 2026. It is intended to contribute to conversations surrounding adult exercise participation in Osteogenesis Imperfecta and to encourage collaboration between community practitioners, clinicians, and researchers.
This report has not undergone peer review and should not be interpreted as a clinical study or treatment guideline.
If you reference this report in presentations, publications, educational materials, or future research, the preferred citation is:
Jacobsen, T. (2026). Community-Based Exercise Coaching in Adults With Osteogenesis Imperfecta: A Practice-Based Observational Report, 2018 to January 2026. #UNBREAKABLE BODY.
Version 1.0
Published: July 2026



